Homehemodialysis is considered a very effective and safe technique for renal replacement therapy for the patients with chronic kidney disease(CKD) in stage 5 D.
CKD represents actually a leading public health problem worldwide due to the increasing Incidence and prevalence . Globally, we consider that the prevalence is around 13.4% and that the population with chronic kidney failure requiring renal replacement therapy is estimated between 4902 and 7083 million.
CKD could be a silent disease without symtoms untill advanced stages which make in some occasions the diagnosis very late, it affects 1/10 in the general population but only 4/100000 will reach ESRD. The disease is related systematicaly with an increase in ESRD and cardiovascular outcomes, and associated with an increase of morbidity and mortality worldwide.
Definition of CKD :
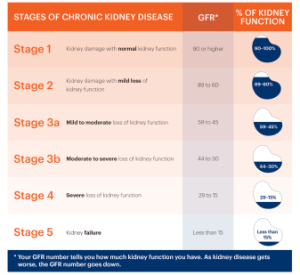
When we consider that a patient is diagnosed and labelled as CKD patient? CKD is defined by a reduced Glomerular filtration rate <60ml/min/1.73m2 and or the presence of markers of renal injury ( Morphological, Histological or Urine and Blood abnormalities : albuminuria, hematuria )for al least 3 months .
Stages of CKD :
The etiological diagnosis is very important and its easier to realize in the initial stages when the patient benefits from a follow Up , when the disease progress and renal atrophia is established its complicated to realize an accurate and clear diagnosis as the lesions are affecting all the structures and the fibrosis
progress. Some simple and basic elements allows to an etiological orientations:
– Anamnesis and Clinical Examination : Edemas, HTA, Purpura, Decrease in urineoutput, foamy urine ( Proteinuria) , Blood in urine ( Hematuria), fatigue, Nausea, Vomiting, loss of appetite…
-Renal Ultrasound and Doppler.
– Proteinuria and Albuminuria.
– Urine spot : Hematuria.
– Autoimmune Parameters.
Main Complications of Chronic Kidney Disease:
A-Cardiovascular Complications:
A1: Hypertension : usually in the ealier stages and its more frequent in glomerulonephritis diseases. Its a major factor in the progression of CKD.
A2: Aterosclerosis and Arterioclerosis: on top of the classical cardiovascular factors : HTA, Dyslipidemia, DM, Age, smoking, CKD has specific factors that increase this risk such as Phosphocalcic Mineral Bone disorders, Hyperhomocysteinemia, anemia, Uremic toxins, Insulin resistance . i would like to highlight that more than 50 % Of the deaths are related with Cardiovascular outcomes in the large sens ( Stroke, Myocardial infarction, peripheral vascular disease..)
A3: Cardiac Implications: Increase Of left Ventricular Hypertrophy , Coronary and vascular calcifications, Uremic cardiopathy, uremic pericarditis.
B-Mineral Bone disorders Characterized by several characteristics :
Secondary Hyperparathyroidism ( excessive production of parathyroid hormon) with a deficit in Vitamin D secondary to the reduction on Renal 1 alpha Hydoxylase activity, Hypocalcemia, Hyperphosphoremia, metabolic acidosis which worsens the bone lesions, Renal osteodystrophy ( osteomalacia secondary to vitamin D deficit and osteoitis fibrosa cystica wich is a disorder involving the bone secondary to hyperparathyroidism)
C- Dyslipidemia:
C1- Hypercholesterolemia mainly related with Nephrotic Syndrom in glomerular diseases. C2-Hypertrygliceridemia mainly related with decrease in HDL cholesterol.
D-Malnutrition : The Dietician Follow Up is very important for the patient with Chronic kidney disease as they arrive to stage 5D and with an important reduction of protein anabolism due to peripherical insulin resistance , an increase in the protein catabolism secondary to the metabolic acidosis, and a decrease intake related with the progressions of CKD. Albumin and prealbumin remains the main
important parameters to monitor in the patients CKD with Diet plan tailored to the patient. E-Hematological complications :
E1: Normocitic Normocromic Arregenerative Anemia due to the lack of synthesis of Erythropoietin our patients present an important fatigue with astenia , Functional Angina ,decrease in the Libido, Increase of LVH. The target for the hemoglobin for the patients CKD in dialysis is between 10/12mg/dl. we are using iron and Aranesp to reach this target and every month we realize laboratory test to optimize the dosis.
E2: Hemorrageas are more frequent in the patients with Chronic Kidney disease due to uremic platelets and abnormal primary hemostasia.
E3: Immunitary deficit characterized by low answer to the vaccinations which justify the importance of receiving the vaccinations in a earlier stage of CKD .
F-Electrolyte disorders:
F1: HydroSaline retention : which favorises HTA and cardiovascular complications as heart failure. Its for this reason that we recommend for our patients in hemodialysis to reduce the water intake and a salt restriction to avoid important interdialytic weight gain and important volume overload.
F2 Hyperkalemia : Hyperkalemia represents a cardiovascular risk and a cause of arrythmia that should be monitored and balanced due to the letal complications . A Hypokalemia diet is recommended for all our patients , the correction of metabolic acidosis, Dialysis sessions respected avoiding skipping the sessions and potassium resin binders are several tools that we use to maintain the potassium in Balance.
How we can prevent it and decrease the speed of progress of a CKD to stage 5 or end stage renal disease? we should focus on the main etiologies of CKD. Diabetes and Hypertension remain the principal causes of kidney failure representing more than 50% of the patient in Dialysis or any other renal replacement therapy option . Obviously there is other Diseases related as Obesity, aging, Glomerulonephritis, autoimmune diseases such a lupus, Vasculitis, Amyloidosis; Lithiasis, Infections, adverse drug reactions, genetic diseases …and the efforts for screening and prevention should be highlighted to decrease the financial costs and the prevalence and incidence of this chronic condition mainly in the patients with high risk as the patients with past medical History (PMH) of HTA, DM, Aged population, recurrent urinary tract infections, urinary lithiasis, congenital or acquired Loss of nephrogenic capital, nephrotoxicity drug exposition, PMH of familar or genetic renal diseases, Autoimmune disease.
Renal replacement Therapy : Homehemodialysis
For the patients not eligible to kidney transplantation or on waiting list , Homehemodialysis is a very efficient and confortable technique for renal replacement therapy . It allows an individualization of the
treatment as per the patient clinical profile.
This Innovative and safe option allows to the patient to realize his medical treatment at home assisted by a nurse or alone . In UAE, we a very honoured to accompany our patients in a multidisciplinary team fully assisted by a very competent and High skilled Nurse team , several Nephrologists, Renal Dieticians
to satisfy the patient needs and provide dialysis at home with an excellent results in terms of clearance , outcomes and quality of life. This Multidisciplinary approach it allows to the patient to continue with an almost normal life with a tailored treatment of hemodialysis at home maintaining to the maximum his daily activities and Routine . The innovation is conceptual and technological as we are using the only machine approved by FDA the american Machine Nxstage.
Nx Stage is offering a low flow dialysate with sterile bags allowing an effective clearance of toxins and recommending more frequent dialysis in short sessions through a portable machines with an important flexibility to realize the sessions whenever and wherever the patient desire .
Homehemodialysis represent actually around 12% of the patients in end stage renal disease in UAE, very close to the percentage in Australia and New Zealand.The clinical benefits of the technique justify the progressive increase in the interest for the therapies at home to decrease the burden of the disease. It started in the early 1960s and the existence on the last years of those new revolutionary machines plus the clinical benefits and the costeffectiveness allow a resurgence of interest in homehemodialysis. I would like to highlight that in USA 40% of the dialysis patients were on hemohemodialysis in 1973 with the old equipment , in fact the lack of suitable equipment was the main reason that the technique stucked untill the apparition of the low flow dialysate machines which are portable and very easy to use.
Different Modalities are proposed : Short daily Homehemodialysis, Conventional Hemodialysis at Home and Nocturnal Hemodialysis.
Several Publications and articles in the New england Journal, Jasn and Blood purifications studied the impact and the advantages of homehemodialysis clinical outcomes in comparison with dialysis in Center and they conclude a very important benefits :
I would like to emphasize that with Homehemodialysis Significant Cardiovascular benefits were noticed an improvement of 12% in the reduction of left ventricular Hypertrophy which is an independent risk factor for cardiovascular events and mortality , 20% fewer Hypotensive episodes during dialysis sessions, 7% decrease in systolic Blood pressure , 32% less antihypertensive Consumed, 11% fewer cardiovascular related admissions, Improvement of restlesslegs syndrome, Improvement of quality of life, Improvement of mental and Physical health , Improvement of apetite , Flexibility and freedom for time treatment, reduction in total admission , maintenance of residual renal function, reduction in Hospitalization cost for transport.
During Covid pandemic, many patients in dialysis in Hospitals were looking for a safe and isolated alternative to realize their chronic treatment avoiding nosocomial infections ( infections that we can catch in the hospital, mainly for the patients with immune deficit, and also to avoid contact with other
patients Covid+), Our programm fulfilled this need as well and we saw the incidence growing during this period.
Regarding to Our results , we studied our epidemiological and Clinical Data during the last year , we had a total patients number of 310 , the average age is 67 years old, 40.45% female and 59.55 % male patients with an average weight of 67.5Kg , 25% were under Long term care facility and the rest realizing hemodialysis at home. Regarding the vascular access 27.42% have AVF ( i would like to emphasize that all the patients were referred to the vascular surgeon for mapping for arteriovenous Fistula and the intervention was not done because of patient refusal or the patient was not eligible due to calcifications and weak venous capital ), 66.4% have Permanent jugular catheter, 1.94% have GraftAVF and finally 4.19% have an AVF on maturation and permanent CVC in the moment of the study.
We asessed all these patients with quality of life questionnaires and we find same benefits prescribed in the articles and the reviews with decrease time for recovery , improvement in sleep and in a scale of 1-10 ,we obtained a rate of 8,67 regarding the Global patient satisfaction .
Clinically I would like to share some of our oustanding results , the main sessions per week is 3,82 sessions per week, with a lenght average of 206.5 min , Flow fraction of 46.31%, Uf volume is around 1.77 Liters per session, BFR average : 343.39ml/Min and dialysate volume of 30 Liters. Our results were in the target required as the sdKT/V is 2.19 . The laboratory results of our patients were excellent , the average of albumin is 36.57 g/l, Calcium corrected per albumin is 2.26mmol/l, Phosphorus 1.7mmol/L,Mg: 1.12mmol/l and hemoglobin was 10.75 g/dl so in target as per KDIGO Guidelines. I would like to highlight that all our clinical protocols follows best practices and international Guidelines.
Those results are the fruit of active follow up and monitoring thanks to the patient compliance, willing to respect the medical prescription and renal diet for dialysis patients and adherence to their medication associated to the multidisciplinary approach by several passionated professionals always present and available for the patient wellbeing to provide the best answer and last technological innovation in dialysis healthcare, incorporating and improving the accessibility to the chronic treatment in a safe environment
Dr Imane Guermah
Nephrologist HHD